
Explore the Four Layers of Continuity and learn how organizations can move from isolated appointments to proactive, visible, continuous care.

Most organizations mistake documentation for continuity of care. Explore the hidden gap between recording care and sustaining it.

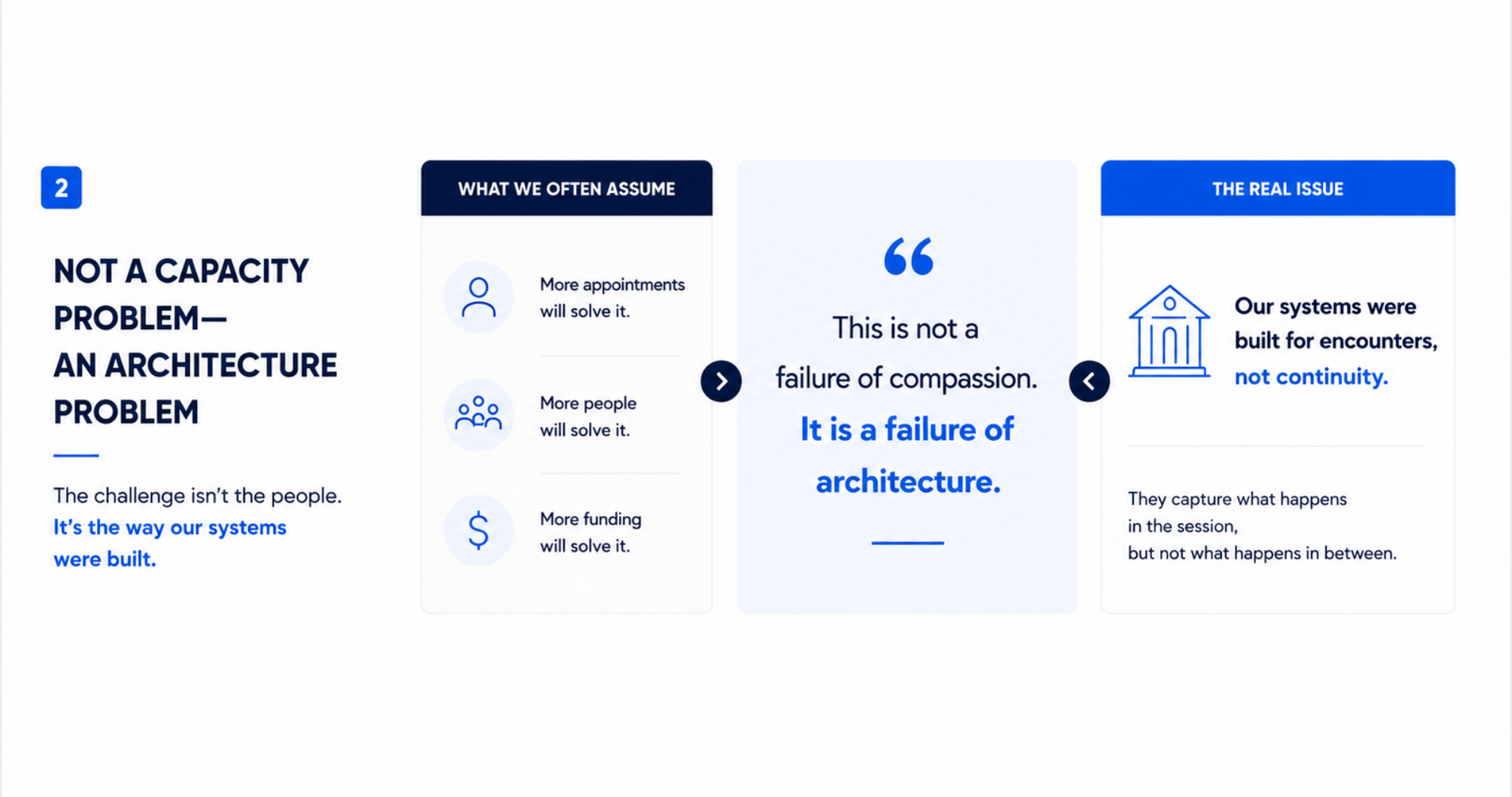
Most emotional struggles happen between appointments. Explore why continuity of care matters beyond sessions.

Mental health support shouldn’t disappear between appointments. Discover how Coming Home is redefining continuity of care through real-time, trauma-informed support.

Explore the hidden gaps between moments of care and why continuity of support matters for real human outcomes. The Space Between Support examines emotional disengagement, provider burnout, and the need for systems that maintain connection between sessions.

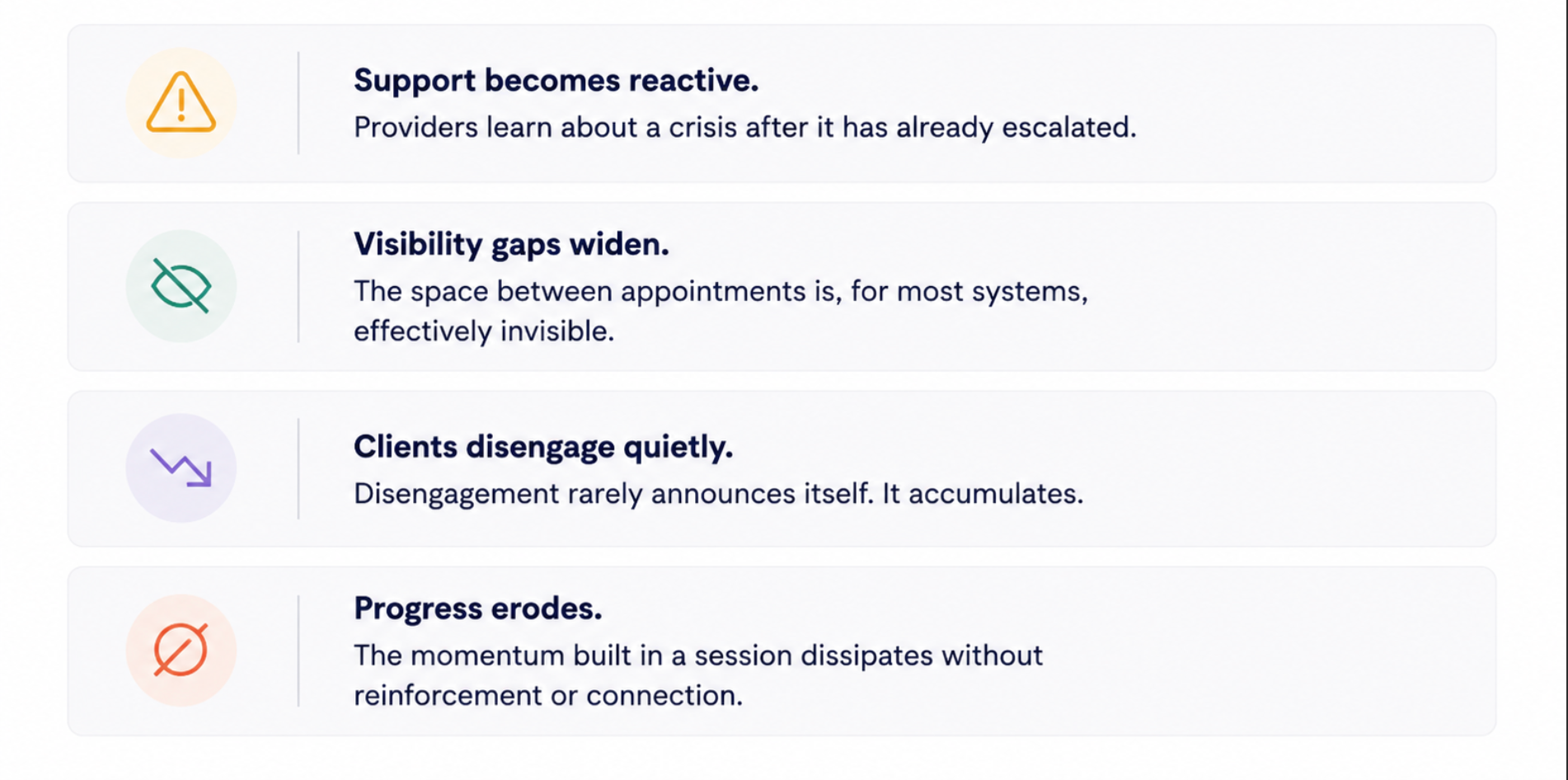
7 Indicators That Reveal Fragmented Care

The moments where engagement is either sustained or quietly lost.
Coming Home cofounder Carlos Wallace reflects on grief, continuity of care, and what actually happens between sessions.
A personal story about growing up unseen by the system and how gaps in information and visibility impact care between moments that matter most, from Coming Home co-founder Chance Glasco.